Walking in History
Ruma - earliest pictorial record of Polio
(3,000 BC)
 Ruma
was a Syrian boy who probably had the earliest known case of a disease
now known as Polio. When Ruma was 5 years old he got very sick with pain
in his head and his leg ached. When he was no better after several days,
his father carried the boy to the temple where they believed the priest
would cure him with powerful magic (charms, amulets, herbs, and magic drinks).
Ruma
was a Syrian boy who probably had the earliest known case of a disease
now known as Polio. When Ruma was 5 years old he got very sick with pain
in his head and his leg ached. When he was no better after several days,
his father carried the boy to the temple where they believed the priest
would cure him with powerful magic (charms, amulets, herbs, and magic drinks).
The story of Ruma is seen on a 3,000 year old Egyptian tablet, and is
perhaps the earliest pictorial record of Polio. Some thought maybe his
leg was just poorly drawn, but the stone tablet (stele) tells the story
of Ruma, now a grown man with a withered right leg. And, he is holding
a long stick to use as a crutch. The tablet tells that he is a gatekeeper
at the temple of Astarte in Egypt. He is shown with his wife, Ama and his
young son, Ptah-m-heb. He brings with him fruit, wine, and a gazelle for
the goddess he believes saved his life.
"Never to Die: the Egyptians in their own words," by Josephine Mayer
and Tom Prideaux, p. 80
"Polio Pioneers, The Story of the Fight Against Polio" by Dorothy and
Philip Sterling, 1955, p. 9-12
The Polio Stele (limestone with original paintwork) is part of museum
collection at the Ny Carlsberg Glyptotek,
Dantes Plads
7, Copenhagen, Denmark, and was acquired in Egypt in the 1980s.
King Narmer (3,200 BC)
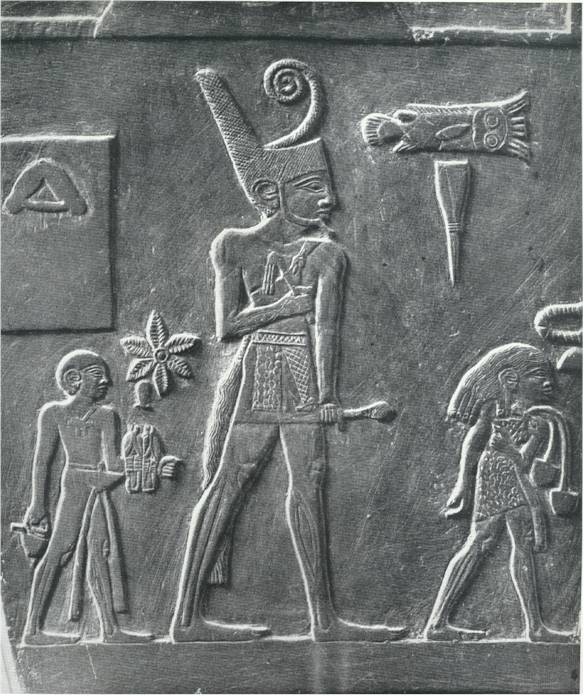
Mighty stride and powerful gastrocnemius and soleus. Scene from the
ceremonial slate (mudstone) palette of Narmer (the last king of Dynasty
0/ or the first king of Dynasty I) discovered at Hierakonpolis, 25º
N 05'; 32º E 47', by Quibell in 1898.
One of the most amazing things about poliomyelitis is that no epidemic
of it was
noted until seventy-one years ago. Large epidemics of other virus diseases,
such as
smallpox, yellow fever, influenza, and measles, are recorded much farther
back in
history.
Greer Williams, Virus Hunters (1960)
No doubt many scenes which occurred in London during the great plague of
1665
were reenacted in our Long Island andWestchester towns. Under the sway
of
panic people looked with skepticism and suspicion on government health
officers.
The selectmen of many villages, whose doctors were struggling with the
impossible
and failing to stop the epidemic or save the individual case from paralysis,
resorted
to home-made martial law. Deputy sheriffs, hastily appointed and armed
with
shot-guns, patrolled the roads leading in and out of towns, grimly turning
back all
vehicles in which were found children under sixteen years of age. Railways
refused
tickets to these selected youngsters, the innocent victims of ignorance
and despair.
Indeed, the notion was firmly held that below the magic age, called sweet
at other
times, there lurked the dread disease, whereas above it no menace existed
either
for the individual or the community.
George Draper, Infantile Paralysis (1935)
The epidemic of 1916 will go down in history as the high-water mark in
attempts at
enforcement of isolation and quarantine measures.
John R. Paul, A History of Poliomyelitis (1971)
It was not the disease itself, but outbreaks of epidemic proportions
that were of recent origin. An Egyptian stele, dating from
the period 1580-1350 BC and depicting a young man with a withered leg
leaning on a long staff, suggests that polio has been endemic since ancient
times.
The term poliomyelitis derives from the Greek words, polios, meaning `grey',
and myelos,
`matter', and refers to the grey matter of the spinal cord. The disease
was called by many names
in the nineteenth and early twentieth centuries, including: Dental Paralysis,
Infantile Spinal
Paralysis, Teething Paralysis, Essential Paralysis of Children, Regressive
Paralysis, Myelitis of the
Anterior Horns, Tephromyelitis (from the Greek tephros, meaning `ash-grey')
and, most
poetically, Paralysis of the Morning-after the way in which a child goes
to bed apparently
healthy, wakes feverish in the night and then is unable to get up in the
morning. The number of
names ÷ and there were several others ÷ reflects the confusion
over the nature of the disease.
Perhaps the earliest recorded case is that of Sir Walter Scott (born in
Edinburgh in 1771),
who was led to believe that he `showed every sign of health and strength'
till he was about
eighteen months old. Then:
One night, I have been told, I showed great reluctance to be caught and
put to bed,
and after being chased about the room, was apprehended and consigned to
my
dormitory with some difficulty. It was the last time I was to show much
personal
agility. In the morning I was discovered to be affected with the fever
which often
accompanies the cutting of large teeth. It held me three days. On the fourth,
when
they went to bathe me as usual, they discovered that I had lost the power
of my
right leg .... There appeared to be no dislocation or sprain; blisters
and other
topical remedies were applied in vain ...
The impatience of a child soon inclined me to struggle with my infirmity,
and I
began by degrees to stand, to walk, and to run. Although the limb affected
was
much shrunk and contracted, my general health, which was of more importance,
was much strengthened by [my] being frequently in the open air, and, in
a word, I
who in a city had probably been condemned to helpless and hopeless decrepitude,
was now a healthy, high-spirited, and, my lameness apart, a sturdy child
...
The first attempt at a clinical description of the disease was made by
the English physician,
Michael Underwood, in the second edition of his treatise on the Diseases
of Children,
published in 1789. He calls it `Debility of the Lower Extremities' and
writes: `It is not a common
disorder, I believe, and seems to occur seldomer in London than in some
parts. Nor am I
enough acquainted with it to be fully satisfied, either, in regard to the
true cause or seat of the
disease, either from my own observation, or that of others.' Nevertheless,
he is inclined to
attribute it to `teething and foul bowels'. Where both lower extremities
`have been paralytic,
nothing has seemed to do any good but irons to the legs, for the support
of the limbs, and
enabling the patient to walk'. (A later editor of Underwood's treatise,
obviously unfamiliar with
the flaccidity of the paralysis resulting from polio, comments parenthetically:
`If the limbs are
paralytic, how are irons to the legs to enable the patient to walk?')
The first account of an outbreak of the disease was written by a young
doctor
called John Badham, the son of a distinguished professor of medicine at
the
University of Glasgow. It took place in 1835 in Worksop, in north
Nottinghamshire. There were four cases, described by Badham in meticulous
detail. He comments on the `extraordinary youth' of all four patients;
on the
`cerebral symptoms', such as drowsiness or abnormality of the pupils of
the eye; on
the `remarkable [fact] that in no one instance has the health of the child
been in any
degree impaired'; and on the strabismus (squinting) apparent in one case,
leading
him `to suspect a cerebral complication, rather than a spinal one'. Unfortunately,
the
thirty-two-year-old John Badham died of consumption in 1840, the very year
in
which the first systematic investigation of poliomyelitis, written partly
in response to
his account of the Worksop outbreak, was published in Germany.
Like Badham, Jacob von Heine draws attention both to the extreme youth
of patients (six
months to three years) and to their good general health (though he is referring
to their health
preceding the attack). But where Badham sees only `drowsiness', Heine recognises
fever and
pain in children during the pre-paralytic phase of the illness, which makes
him think that the
disease may be contagious, and far from suspecting `a cerebral complication,
rather than a spinal
one', he finds no cerebral involvement and concludes that all the symptoms
`point to an affection
of the central nervous system, namely the spinal cord'.
In the matter of treatment (which had baffled Badham), Heine steered clear
of fashionable
nostrums such as purges, emetics, blisters and bleedings, and recommended
`exercise, baths,
and various simple surgical procedures, followed by the application of
braces and apparatus'. As
the historian of the disease and a leading participant in its `conquest',
Dr John R. Paul of Yale
University points out, `Considering the degree to which the handling of
a given disease is wont to
change over a period of 125 years, Heine's treatment of paralyzed limbs
and the resulting
deformities and disabilities of children has undergone remarkably little
alteration.'
In 1907 the Swedish paediatrician, Ivar Wickman, named the disease `Heine-Medin
disease'
after both the great German orthopaedist and the Swedish pioneer, Karl
Oskar Medin, whose
pupil Wickman was. Medin's involvement in an unprecedented outbreak of
forty-four cases in
Stockholm in 1887 led him to categorise various types of the disease ÷
spinal, bulbar, ataxic,
encephalitic and polyneuritic ÷ as well as, crucially, to conclude
that its acute phase consisted of
two separate fevers, sometimes with a fever-free remission (what the American
doctor George
Draper mis-labelled the `dromedary form' ÷ it is the Bactrian camel,
not the dromedary, that
has two humps). The initial fever was no more than a general malaise; it
was the second attack
that did the damage to the central nervous system.
The significance of this finding was not lost on the young Ivar Wickman
when he came to
investigate the infinitely more serious Scandinavian epidemic of 1905,
in which there were more
than 1,000 cases. The questions that concerned him were: was the disease
contagious and, if so,
how was it spread ÷ by direct contact with infected children, or
by carriers of the virus who
themselves showed no sign of infection? Others, including On Charles Caverly
in his notes on the
1894 Vermont outbreak, had observed that there could be `abortive' or non-paralytic
cases.
Wickman's originality lay in suggesting that non-paralytic cases were both
far more widespread
than anyone had supposed and instrumental in spreading the disease. His
experience of the 1905
epidemic convinced him that Heine-Medin disease was highly contagious,
and that apparently
healthy or only mildly affected persons played a key role in spreading
it.
Although he committed suicide at the age of forty-two, just two years before
the New York
epidemic, Wickman's historic monograph of 1907 earned him a place in the
Polio Hall of Fame
erected in 1958 at Warm Springs, Georgia, to celebrate the twentieth anniversary
of the
National Foundation for Infantile Paralysis (where fifteen doctors and
scientists are honoured,
along with the founders of the NFIP, Franklin D. Roosevelt and Basil O'Connor).
The end of the nineteenth and the beginning of the twentieth century was
once considered a
medical golden age, but has recently been dubbed `the Childhood of Scientific
Medicine, a
period of great stimulus and rapid growth, filled with the excitement of
learning new things ÷
and also filled with childish certainties'. Following Robert Koch's painstaking
and brilliant work
on anthrax, tuberculosis and cholera, and Pasteur's discovery of a rabies
vaccine (a century after
Jenner had started the whole business of vaccination by deliberately infecting
people with
cowpox as a preventive of smallpox), `Everybody, everywhere, tried to hunt
microbes, see
them, grow them, identify them, explain them, escape them. Their primary
activity ... was finding
and naming the causes of infectious diseases. It was the Day of Diagnosis.'
The microbes being
so assiduously hunted were largely bacteria, and the essential tackle needed
for their capture
included the microscope, dyes that highlighted the microorganisms, culture
dishes, test tubes and
some unfortunate laboratory animal to act as involuntary host. Bacteriology,
or microbiology,
was the name of this sport; virology had yet to be born.
As far as microbe hunters were concerned, the only difference between bacteria
and viruses
was one of size. Bacteria were the organisms which would not pass through
a porcelain filter;
viruses the ones which would. If the filtration process succeeded in sterilising
cultures of
organisms, then they were bacteria; if not ÷ and laboratory animals
could be reinfected after
filtration of the culture ÷ it was called a virus. Bacteria became
visible under the microscope if
stained with certain types of dye; viruses, however, were too small to
be seen, even through an
optical microscope, and it was practically impossible to study them visually
before the invention
of the electron microscope in 1937.
Despite the virtual invisibility of viruses, immunisation was first discovered
in relation to a virus
÷ smallpox ÷ and the first two human vaccines (the second
being rabies) were virus vaccines.
But as John Rowan Wilson points out, `almost all the really productive
developments in this field
after the death of Pasteur until 1930 were in connection with bacteria.
The reason for this lay in
the technical difficulties of culturing the organisms'. In Vienna in 1908,
Drs Karl Landsteiner and
Erwin Popper discovered that the infectious agent for poliomyelitis was
not a bacterium, but a
`filterable virus' ÷ as any micro-organism that passed through the
porcelain filter came to be
called. When Landsteiner and Popper injected filtered fluid taken from
the spinal cord of a polio
victim into the brains of two monkeys, both animals went down with the
disease. Through their
experiment, the two scientists not only established the cause of polio,
but also set the pattern for
future research, with monkeys as polio's primary `guinea pigs'.
The importance of their discovery was widely recognised, not least by Simon
Flexner in New
York. Flexner had been appointed director of the newly established Rockefeller
Institute for
Medical Research in 1903 and had already successfully developed an antiserum
(serum is the
watery fluid left when blood coagulates and contains proteins called globulins
which comprise
antibodies) for cerebrospinal meningitis. In doing this, he had worked
out one of `only about four
big ideas [needed] in order to prevent human diseases via vaccination'.
The first big idea, at least two thousand years old, is that people who
recover from
certain infectious diseases are safe from a second attack. The second is
that a
scientist can find a suitable animal host, susceptible to the infection,
that will
manufacture virus for him in quantity. The third idea is that in such a
host, or
through some laboratory manoeuvre, the scientist can find a way of taming,
stunning, or killing the virus so that it will still produce disease resistance
but not the
disease. The fourth idea is the use of antibodies in an immune serum ÷
or
antiserum, as it is also called ÷ as a quantitative index for virus
presence. This is
called a virus-neutralization test.
The neutralisation test was originated by George M. Sternberg, a military
doctor who was
promoted to Surgeon General of the US army during Cleveland's presidency.
It was already
known that blood serum contained antitoxic properties in relation to bacteria,
but Sternberg was
the first to show that it was true for viruses, too. Following Sternberg's
÷ and Landsteiner's ÷
lead, Flexner `demonstrated in 1910 that the serum of monkeys convalescent
from experimental
[i.e. artificially induced] poliomyelitis contained antibodies, spoken
of as "germicidal substances"
÷ a finding that was made almost simultaneously by Landsteiner and
others'.
Shortly after this, Netter and Levaditi [in Paris] and others also found
these
neutralizing substances in the blood of humans recovering from poliomyelitis.
This
demonstration of antibodies in convalescent patients was to prove another
landmark in the therapeutic history of the disease. Its significance ranked
almost on
a par with the discovery of the virus, a fact unappreciated until some
years later.
One of several sons of Jewish immigrant parents, Simon Flexner had had
a distinctly unpromising
childhood in Louisville, Kentucky. When he was ten, his father, Morris,
had taken him along to
the local jail as a tacit warning of what lay ahead of him if he did not
mend his ways. But this visit
filled the young Flexner with excitement rather than dread and he surprised
his older brothers,
who had gathered round to gloat over his humiliation, by saying that he
had `had a swell time'.
He left school at fourteen and was apprenticed to a plumber, according
to one historian, who
writes: `At the end of a week the plumber returned him to his father with
the blunt evaluation that
he was too dumb to be a plumber.' It is a good story, perhaps too good,
since Flexner's son tells
it rather differently:
Simon received a curt command to follow his father and was led into a plumber's
shop. Morris pushed the boy forward and offered him to the plumber as an
apprentice. The plumber said he did not need an apprentice. Morris went
out and
walked off, leaving the boy standing on the street.
Whichever version one accepts, there can be no doubt that during his adolescence
Flexner was,
in his own words, `in and out of wretched jobs leading nowhere'. It was
not until he was
apprenticed to a pharmacist that he found a sense of direction. After that,
his rise was meteoric,
through Johns Hopkins Medical School in its heyday and a professorship
of pathology at the
University of Pennsylvania to the Rockefeller Institute, whose first director
he was ÷ a post he
held for more than thirty years. Considering the ÷ perhaps disproportionate
÷ influence he
would have on medical research in the United States over three decades,
it is worth noting that
his initial medical education at the University of Louisville Medical School
was a farce. Flexner
recalls, `I did not learn to practice medicine, indeed, I cannot say that
I was particularly helped
by the school. What it did for me was give me the MD degree.' Appropriately
enough, his own
younger brother, Abraham, was to put an end to such anomalies by exposing
them in his 1910
`Flexner Report' on Medical Education in the United States and Canada.
Simon Flexner's lack of clinical competence and experience, combined with
his belief that
`medicine derived from such basic sciences as pathology, physiology, chemistry,
and
bacteriology', meant that his initial staff appointments to the Rockefeller
Institute `were not of
physicians interested in pursuing problems in clinical medicine, but rather
of investigators skilled
in the basic sciences who sought to cast light on medical problems through
experimental
research'. The success of the institute's experiments with monkeys in developing
the antiserum
for cerebrospinal meningitis, reducing the mortality rate from three in
four to one in four,
convinced Flexner of the validity of his methods and determined his approach
to polio research,
encouraging a degree of confidence which was scarcely justified by subsequent
events.
Initially, however, he succeeded in taking Landsteiner's work a crucial
stage further by
transferring poliovirus not just from humans to monkeys, but from monkey
to monkey. (Others,
including Landsteiner himself, also achieved this, but Flexner did it first.)
When Flexner published
his report, he omitted the word experimental from the title ÷ a
very significant omission,
according to Dr John Paul:
Indeed this was a major mistake that was to dog Flexner's footsteps throughout
his
entire professional life ÷ his failure to distinguish between certain
aspects of
experimental poliomyelitis in the monkey and the disease in man ... It
was an error
with unfortunate implications that were to influence thought at the Rockefeller
Institute for a generation.
Paul compares Flexner's role as `laboratory doctor' unfavourably with the
clinical investigations
of a contemporary Swedish team headed by Carl Kling. Sweden had suffered
another epidemic
in 1911 (at nearly 4,000 cases the largest to date anywhere in the world),
and Kling and his
colleagues succeeded in isolating poliovirus from living patients ÷
not just from those who had
been paralysed, but from abortive cases as well, thus confirming Wickman's
theories about the
way the disease spread. From autopsies they also made important discoveries
of the sites in the
body favoured by the virus other than the central nervous system, where
the damage was done;
as they expected, they found it in the throat, but they were surprised
to find it in the intestinal wall
as well. This caused them to ponder such key questions as how the virus
entered the body and
how, once there, it penetrated the central nervous system. They did not
come up with all the
answers but, by combining clinical and laboratory techniques, at least
they were asking the right
questions.
A news item in the New York Times of 9 March 1911 suggests that Simon Flexner
was so
confident of the rectitude of his approach that he was not looking to the
Swedes or anyone else
for help in solving the mysteries of polio:
The Rockefeller Institute in this city believes that its search for a cure
for infantile
paralysis is about to be rewarded. Within six months, according to Dr Simon
Flexner, definite announcement of a specific remedy may be expected.
`We have already discovered how to prevent the disease,' says Dr Flexner
in a
statement published here today, `and the achievement of a cure, I may
conservatively say, is not now far distant ...'
No cure for polio has ever been achieved and more than forty years would
elapse before a safe
and reliable method of prevention was developed.
During the 90's Edward Hooper, a British journalist, traveled to Africa
and became convinced that AIDS was an act of man, not an act of God. He
interviewed hundred of participants and collected thousands of documents
to support his theory. The earliest cases of AIDS occurred in central Africa,
in the same regions where Koprowski's vaccine was given to over a million
people in 1957-1960.
Hooper mapped the locations where Koprowski's CHAT vaccine was given
and where the earliest cases of AIDS were discovered. It showed a dramatic
geographical correlation.
Hooper claims that kidneys from chimpanzees infected with SIV were used
to grow the polio virus during Koprowski's 1950's vaccination campaign.
Archival footage confirms that a large number of chimpanzees were housed
at Camp Lindi, located upstream from Koprowski's medical laboratory in
Stanleyville in the former Belgian Congo.
Paul Osterrieth and Hilary Koprowski steadfastly denied that chimpanzee
tissue was used to grow the polio virus in the Congo.
Before his death Pierre Doupagne, the chief technician at the laboratory
of Stanleyville admitted to Edward Hooper that he made sterile tissue culture
from chimps for Paul Osterrieth.
In September 2000 the world's top AIDS specialists assembled at London's
Royal Society for a conference on the origins of AIDS. It was meant to
give Edward Hooper a chance to present his evidence to the scientific community.
From the opening of the conference arguments were launched against Hooper's
theory. Then there was was a surprise announcement. Samples of Kopowski's
CHAT vaccine had been located and tested and found not to have any trace
of HIV, SIV or chimp DNA.
This announcement was viewed by the scientific community as a decisive
statement against Hooper's theory. Articles were published in Nature and
Science concluded that Hooper's hypothesis was not viable.
The Emperor Claudius (reigned 41 - 54AD)
 Emperor
Tiberius Claudius Drusus Nero Germanicus was born in 10 BC to Nero Claudius
Drusus and his wife
Emperor
Tiberius Claudius Drusus Nero Germanicus was born in 10 BC to Nero Claudius
Drusus and his wife
Antonia. Although he came from a royal blood
line, his family had a very low opinion of his abilities and often
ignored him. Labeled an invalid from birth
because of physical disabilities including partial paralysis, stammering,
slobbering, and limping, he was the last person
his family thought would inherit the throne and serve as Roman
Emperor. An outcast in his home environment,
Claudius turned to the study of history to occupy his time. He
authored various works about orthographic
reform of the Roman alphabet and a work defending Cicero, a
republican politician and orator. Claudius
also enjoyed playing dice games.
 Claudius
escaped the wrath of his mad nephew, Caligula, because the effects of his
infantile paralysis (polio) made him appear as no threat to the throne.
However, after the Praetorian Guard assassinated Caligula and he was thrust
upon the throne, he
Claudius
escaped the wrath of his mad nephew, Caligula, because the effects of his
infantile paralysis (polio) made him appear as no threat to the throne.
However, after the Praetorian Guard assassinated Caligula and he was thrust
upon the throne, he
surprised everyone by being a capable administrator. His major mistake
was recalling Caligula's sister Agrippina back from
banishment and wedding her. She later poisoned him after he adopted
her son Nero, to get her son on the throne.
Claudius' rise to power came after Emperor
Gauis (Caligula), his nephew, was unexpectedly murdered on January
1, AD 41. Claudius became heir to the throne,
to many a Roman's dismay. The soldiers, courtiers, freedman, and
foreigners were his main support although
the senatorial aristocracy also offered to back the new emperor. Many
Romans sought to have Claudius assassinated
because of his cruel and ruthless discussions and actions with
members of the senate and knighthood. It is
thought by some that he even executed senators on occasion. Despite
this conflict Claudius did respect these agencies
and gave new opportunities to them both.
Claudius' reign was marked with an expansion
of the Roman Empire. He invaded and conquered Britain in AD 43
and captured Camulodunum. There he started
a colony of veterans and built client-kingdoms to protect the small
populated land. Claudius also took over North
Africa and annexed Mauretania, where he established two
provinces as well. Around AD 49 he also annexed
Iturea and allowed the province of Syria to control it, trying
not to come into conflict with the Germans
and the Parthians.
In the area of civil administration he encouraged
urbanization. The judicial system improved under his reign and he
favored the modern extension by individual
and collective grants in Noricum. Claudius also made many
administrative innovations. He increased his
control over finances and province administration and gave
jurisdiction of fiscal matters to the governors
under him in the senatorial provinces.
Claudius' personal life was wrought with conflicts
that ultimately led to his undoing. He married three times. His
first wife, Boudicca, started a revolt, and
his second wife had a strong sexual appetite that led her to conspiracy
and ultimately, her execution. Claudius' third
time was not a charm either. He decided to stay within the family and
married his niece, Aggripina. She was very
influential over Claudius to the point where he adopted her son Nero.
Then she fed Claudius a dinner containing
poisonous mushrooms which killed him. Her main motive was that her
precious son, Nero, might inherit the throne.
Although Claudius was generally thought of
as a weak leader and was labeled, even by his own family, as
someone not worthy to rule; he made notable
contributions to the development of the Roman empire. He
conquered and colonized Britain, established
provinces in North Africa, and he urbanized and innovated his civil
administration. He died an unnecessary and
tragic death by a plate of poisonous mushrooms dished out by his scheming,
power-hungry wife.and was succeeded by his adopted son, Nero.
The medical and historical evidence suggest that Claudius was given
mushrooms that contained muscarine, a deadly toxin that
attacks the nervous system, causing a wide range of agonizing symptoms,"
says William A. Valente, M.D., clinical professor of
medicine at the University of Maryland School of Medicine.
On October 13, AD 54, Claudius became gravely ill after devouring a
heaping helping of mushrooms served up by his fourth
wife, Agrippina. His symptoms included extreme abdominal pain, vomiting,
diarrhea, excessive salivation, low blood pressure,
and difficulty breathing. Claudius was dead within 12 hours.
So what was Agrippina's motive? "Power," says Richard Talbert, Ph.D.,
who is the William Rand Kenan Professor of History
at the University of North Carolina, Chapel Hill. Ambitious and influential,
Agrippina had convinced Claudius to adopt her son
Nero, so that Nero would inherit the throne. But when Agrippina learned
that Claudius might tap his own son for the job,
Agrippina hatched the mushroom murder plot.
Some historians have suggested that Claudius' demise was hastened by
an additional dose of poison administered by his
physician. "That's pure speculation," says Dr. Talbert, who notes that
the historical record is far from complete. While the
weapon of choice was the poisoned mushrooms, Dr. Valente says Claudius
may actually have died of "de una uxore
nimia,"---a Latin phrase meaning "one too many wives."
Some say that Claudius also gives his name to the symptom of intermiittent
claudication, pathognomonic of peripheral vascular disease. He had a limp
together with a tendency to stop walking and grimace as if in pain. The
two words however, are etymologically unrelated. There already existed
a latin word at the time 'claudeo/claudico' which meant to limp, which
seems a rather cruel coincidence for the Emperor. Claudicant first appeared
in the English language in 1624.
Autobiography,
translated by Robert Graves
Tamerlane (1336 - 1405) - The Iron Limper
-
Tamerlane, the name was derived from the Persian Timur-i
lang, "Temur the Lame" by Europeans during the 16th century. His Turkic
name is Timur,
which means 'iron'. In his life time, he has conquered more than anyone
else except for Alexander. His armies crossed Eurasia from Delhi to Moscow,
from the Tien Shan Mountains of Central Asia to the Taurus Mountains in
Anatolia. From 1370 till his death 1405, Temur built a powerful empire
and became the last of great nomadic leaders.
There are abundant ancient sources written about Tamerlane. We have
the primary source from Spanish Ruy Gonzalez de Clavijo, sent by King Henry
III of Castile on a return embassy to Tamerlane. There is also a Persian
biography of Tamerlane by Ali Sharaf ad-Din and the Arab biography by Ahmad
ibn Arabshah; from Marlowe to Edgar
Allan Poe, he continues to fascinate us as hero or viper.
Timur claimed direct descent from Jenghiz Khan through the house of
Chagatai. He was born at Kesh (the Green city), about fifty miles south
of Sarmarkand in 1336, a son of a lesser chief of the Barlas tribe. Sharaf
ad-Din explained that in his 20s, he received arrow wounds in battle while
stealing sheep in his twenties and left him lame in the right leg and with
a stiff right arm for the rest of his life. But Tamerlane made light of
these disabilities; by 1369 he had possessed himself of all the lands which
had formed the heritage of Chagatai and, after being proclaimed sovereign
at Balkh, made Samarkand his capital.
He was said to be tall strongly built and well proportioned, with
a large head and broad forehead. His complexion was pale and ruddy, his
beard long and his voice full and resonant. Arabshah describes him approaching
seventy, a master politician and military strategist:
steadfast in mind and robust in body, brave and fearless, firm
as rock. He did not care for jesting or lying; wit and trifling pleased
him not; truth, even were it painful, delighted him.....He loved bold and
valiant soldiers, by whose aid he opend the locks of terror, tore men to
pieces like lions, and overturned mountains. He was fautless in strategy,
constant in fortune, firm of purpose and truthful in business.
 In 1941,
the body of Tamerlane was permitted to be exhumed by a Russian scientist,
M. M. Gerasimov. The scientist found Timur, after examining his skeleton,
a Mongoloid man about 5 feet 8 inches. He also confirmed Tamerlane's lameness.
In his book The Face Finder, Gerasimov explains how he was able
to reconstruct exact likenesses of Timur from a careful consideration of
his skull.
In 1941,
the body of Tamerlane was permitted to be exhumed by a Russian scientist,
M. M. Gerasimov. The scientist found Timur, after examining his skeleton,
a Mongoloid man about 5 feet 8 inches. He also confirmed Tamerlane's lameness.
In his book The Face Finder, Gerasimov explains how he was able
to reconstruct exact likenesses of Timur from a careful consideration of
his skull.
Different sources indicate that Timur is a man with extraordinary intelligence
- not only intuitive, but intellectual. Even though he did not know how
to read or write, he spoke two or three languages including Persian and
Turkic and liked to be read history at mealtimes. He had aesthetic appreciation
in buildings and garden. It has been said that he loved art so much that
he could not help stealing it! The Byzantine palace gates of the Ottoman
capital of Brusa were carried off to Samarkand, where they were much admired
by Clavijo. Ibn Khaldun, who met him outside Damascus in 1401 worte:
"This king Timur is one of the greatest and mightiest kings...he
is hightly intelligent and very perspicacious, addicted to debate and argument
about what he knows and also about what he does not know!"
Known to be a chess player, he had invented a more elaborate form of
the game, now called Tamerlane
Chess, with twice the number of pieces on a board of a hundred and
ten squares.
The same as Jenghiz Khan, Timur rose from a nomad ruler; however unlike
Jenghiz Khan, he was the first one based his strength on the exploitation
of settled populations and inherited a system of rule which could encompass
both settled and nomad populations. Those who saw Timur's army described
it as a huge conglomeration of different peoples - nomad and settled, Muslims
and Christians, Turks, Tajiks, Arabs, Georgians and Indians. Timur's conquests
were extraordinary not only for their extent and their success, but also
for their ferocity and massacres. The war machine was composed of 'tumen',
military units of a 10,000 in the conquered territories. It consisted of
his family, loyal tribes particularly the Barlas and Jalayir tribes, recruited
soldiers from nomadic population from as far as the Moghuls, Golden Horde
and Anatolia, and finally Persian- speaking sedentarists.
Timur and his army were never at rest and neither age nor increasing
infirmity could halt his growing ambitions. In 1391 Timur's army fought
and won in the great battle of Kanduzcha on June 18. Following his campaign
in India, he acquired an elephant corps and took them back to Samarkand
for building mosques and tombs. He led the attack and victory on the Ottoman
army in the battle of Ankara on July 28 1402.
With great interest in trade, Timur had a grand plan to reactivate the
Silk Road, the central land route, and make it the monopoly link between
Europe and China. Monopolization was to be achieved by war: primarily,
against the Golden Horde, the master of principal rival, the northern land
route; secondarily, against the states of western Persia and the Moghuls
to the east in order to place the Silk Road under unified control politically;
and finally agaist India, Egypt and China. 
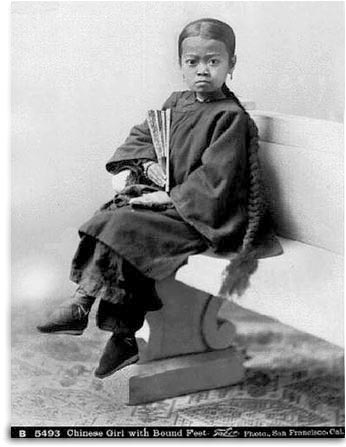
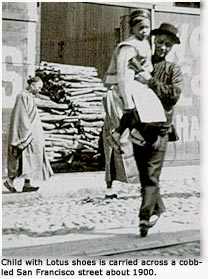 The
Chinese custom of foot binding is another curious reminder of the relationship
between the foot and sex. Strapping of the foot with means of tight bandages
over a period of two or three years was needed to engender the desired
effect. Traditionally, foot-binding began between the ages of five and
seven. Pain was most severe during the first year but gradually diminished.
During the binding the girl at night lay across the bed, putting her legs
on the edge of the bedstead in such a manner as to make pressure under
the knees, thus numbing the parts below. The feet were unbound only once
a month, and the foot was often found gangrenous and ulcerated, with one
or two toes not infrequently being lost. The aim of the ordeal was to produce
a ãthree-inch golden lotusä. The practice, began in the Tang
Dynasty (923-936 AD), continued until the communist era: a 1997 UC San
Francisco study of women over 70 in Beijing found 50% had bound foot deformities.
In 1998, the Xinhua News Agency announced that the Zhiqiang Shoe Factory,
the last to manufacture shoes for bound-feet women would henceforth only
make them on a special-order basis. The factory had added small shoes for
old women to its product range in 1991 to fill a gap in the market, which
was at that time focused on high-heeled shoes.
The
Chinese custom of foot binding is another curious reminder of the relationship
between the foot and sex. Strapping of the foot with means of tight bandages
over a period of two or three years was needed to engender the desired
effect. Traditionally, foot-binding began between the ages of five and
seven. Pain was most severe during the first year but gradually diminished.
During the binding the girl at night lay across the bed, putting her legs
on the edge of the bedstead in such a manner as to make pressure under
the knees, thus numbing the parts below. The feet were unbound only once
a month, and the foot was often found gangrenous and ulcerated, with one
or two toes not infrequently being lost. The aim of the ordeal was to produce
a ãthree-inch golden lotusä. The practice, began in the Tang
Dynasty (923-936 AD), continued until the communist era: a 1997 UC San
Francisco study of women over 70 in Beijing found 50% had bound foot deformities.
In 1998, the Xinhua News Agency announced that the Zhiqiang Shoe Factory,
the last to manufacture shoes for bound-feet women would henceforth only
make them on a special-order basis. The factory had added small shoes for
old women to its product range in 1991 to fill a gap in the market, which
was at that time focused on high-heeled shoes.

Walking in military history
According to the historian Mary Mosher Flesher, a research associate at
Smith College in
Northampton, Massachusetts, locomotion research was the key to
military success in the
eighteenth and nineteenth centuries. Soldiers of that era could
no longer afford to fling
themselves at one another in a furious melee, Flesher points
out in a recent paper in Annals
of Science. Thanks to the invention of muskets, foot soldiers
could now pick off cavalry from
a distance, and battles were decided by marching speed and rate
of fire. "An
eighteenth-century battle was like a chess game," Flesher says.
"The armies didn't always
want to meet and fight. They were trying to get around each other,
to establish positions as
quickly as possible."
Rather than waste time aiming their inaccurate muskets, soldiers
formed tight ranks, shot in
the general direction of the enemy and then dropped back to reload
while the row behind
them advanced. To help soldiers carry out all those actions as
efficiently as possible, an
empirical military science of marching was developed.
Marching theory, Flesher writes, treated a regiment as a mechanical
system, carefully
quantifying the length and cadence of each soldier's step and
the movement of bodies
through space. The first musket drills were developed by the
Dutch in the late sixteenth
century, but they reached an apex of precision among the Prussians
of the mid-eighteenth
century. On the basis of battlefield observations, Frederick
the Great's soldiers were taught
to stand erect yet relaxed and to swing their legs stiffly as
they marched. To synchronize
their movements they stamped their heels on the ground and clapped
their gun barrels in
unison, while drill sergeants timed their steps with stopwatches.
Prussian martinets are a modern-day caricature. But they were
once a military wonder. "The
more I read about them, the more I marvel at how much they knew,"
Flesher says. "Frederick
was able to increase the marching rate from six to twelve miles
a day. His troops could cross
the battlefield obliquely, in step, while their foes were still
moving at right angles." In 1763,
when the Prussians defeated France and its allies in the Seven
Years' War, they owed their
triumph, in part, to better walking. As a result, the single-mindedness
and discipline of
military drills became a blueprint for everything from manliness
to philosophy to political
authority in Prussia.
Marching theory had many of the earmarks of objective research: it was
precise and its
results were reproducible; it was rigorously tested and continually
reexamined. But it took
civilians to create a true science of locomotion--one that applied
to more than just the
battlefield. Beginning in the 1820s, Eduard, Wilhelm and Ernst
Heinrich Weber, three German
brothers with backgrounds in physiology, anatomy and mechanics,
established the world's
first movement laboratory. The Webers used Hanoverian soldiers
as subjects, but they tried
to make the soldiers forget their training: they wanted to study
natural walking, not
marching. In their 1836 book, Mechanics of the Human Walking
Apparatus, the Webers
described the undulations of the spine, the inclination of the
pelvis and the effects of wind
and gravity on the body. Their conclusion--that the body's natural
gait is more efficient than
marching in most situations--brought walking science full circle.
By the early nineteenth century, in any case, precise marching
had lost some of its military
value. Guns had become more accurate and easier to load, and
so soldiers were advised to
take time to aim. Massive regiments had become easy targets.
Skirmishing was now the
order of the day, and Native American hunters were the new model
soldiers. The Webers'
defense of natural walking, in other words, fit the times perfectly.
The Age of Reason, with
its perfectly ordered armies, had given way to the romantic age,
with its emphasis on
individualism, improvisation and feel for terrain. Locomotion
research would gradually fade to
the background, into biomechanics and orthopedics labs, no longer
destined to turn the tides
of war.
Science World Jan-Feb, 1998
Mary Mosher Flesher (1997) Repetitive order and the human walking apparatus:
Prussian military science versus the Webers' locomotion research Annals
of Science 54 (5) 463-487.
Discalced
(Lat. dis, without, and calceus, shoe).
A term applied to those religious congregations of men and women, the
members of which go entirely unshod or wear sandals, with or without other
covering for the feet. These congregations are often distinguished of this
account from other branches of the same order. The custom of going unshod
was introduced into the West by St.
Francis of Assissi for men and St.
Clare for women. After the various modificiations of the Rule of St.
Francis, the Observantines adhered to the primitative custom of going unshod,
and in this they were followed by the Minims and Capuchins. The Discalced
Franciscans or Alcantarines, who prior to 1897 formed a distinct branch
of the Franciscan Order went without footwear of any kind. The followers
of St. Clare at first went barefoot, but later came to wear sandals and
even shoes. The Colettines and Capuchin Sisters returned to the use of
sandals. Sandals were also adopted by the Camaldolese monks of the Congregation
of Monte Corona (1522), the Maronite Catholic monks, the Poor Hermits of
St. Jerome of the Congregation of Bl. Peter of Pisa, the Augustinians of
Thomas of Jesus (1532), the Barefooted Servites (1593), the Discalced Carmelites
(1568), the Feuillants (Cistercians, 1575), Trinitarians
(1594), Mercedarians
(1604), and the Passionists. (See FRIARS MINOR)
STEPHEN M. DONOVAN
Transcribed by Christine J. Murray
Pace Sticks

The Royal Regiment of Artillery (UK) claim to be the originator of the
pace stick. It was used by field gun teams to ensure correct distances
between the guns. This pace stick was more like a walking stick, with a
silver or ivory knob. It could not be manipulated as the more usual pace
sticks, as it was opened like a pair of callipers. Th stick was later developed
as an aid to drill. In 1928, the late Arthur Brand MVO MBE developed a
drill for pace sticks. The stick that he used is still kept in the Warrant
Officers and Sergeants mess at the Royal Military Academy Sandhurst.
 In 1952 the
Academy Sergeant Major (the late John Lord MVO MBE) started a ãpace
sticking competitionä. This competition was held annually between
Royal Military Academy Sandhurst and the Guards Depot. It was originally
four Sergeants in the team and a Warrant officer as the team captain who
acted as the driver and gave the words of command over the course
which involved marching in slow and quick time whilst alternating turning
the stick with the left or right hand. The teams are now modified to a
frontage of three Sergeants but the driver still remains a Warrant Officer.
Since the closing of the Guards Depot in April 1993 the annual competition
has demised, however the All Arms (World Championships) pace sticking competition
still carries on and is held annually at Royal Military Academy Sandhurst.
Teams from all over the world compete in different categories for the title
of World Champion Pace Sticking team or the prestigious individual World
Pace Stick Champion.
In 1952 the
Academy Sergeant Major (the late John Lord MVO MBE) started a ãpace
sticking competitionä. This competition was held annually between
Royal Military Academy Sandhurst and the Guards Depot. It was originally
four Sergeants in the team and a Warrant officer as the team captain who
acted as the driver and gave the words of command over the course
which involved marching in slow and quick time whilst alternating turning
the stick with the left or right hand. The teams are now modified to a
frontage of three Sergeants but the driver still remains a Warrant Officer.
Since the closing of the Guards Depot in April 1993 the annual competition
has demised, however the All Arms (World Championships) pace sticking competition
still carries on and is held annually at Royal Military Academy Sandhurst.
Teams from all over the world compete in different categories for the title
of World Champion Pace Sticking team or the prestigious individual World
Pace Stick Champion.
Military Stride Length & Cadence
|
Speed
|
Steps per minute
|
Distance
per minute |
Step Length
|
| Slow |
75 |
62 yds 18 ins |
30" |
| Quick |
110 |
91 yds 24 ins |
30" |
| Double |
150 |
150 yds |
36" |
| Side |
Quick time |
- |
10" |
| Stepping out |
Slow or Quick
time |
- |
33" |
| Stepping short |
Slow or Quick
time |
- |
10" |
| Side pace to
clear or cover another (as in forming four deep) |
- |
- |
21" |
In order to beat the time correctly on a drum the "Plummet" must be
used. A variety of pendulums or plummets have been constructed for this
purpose. When none of these can be procured, the following simple method
can be adopted. Suspend a spherical ball of metal by a string that is not
liable to stretch; the length of the string measured from the point of
suspension to the centre of the ball, must be as follows for the different
degrees of march. Thus arranged, the plummet will swing the exact time
required.
|
Inches |
Hundreths |
| Slow time |
24 |
96 |
| Quick |
11 |
66 |
| Double |
6 |
26 |
In comparison to the 120 steps/minute pace of other French units, the
Foreign Legion has an 88 steps/minute marching pace. This can be seen at
ceremonial parades and public displays attended by the Legion, particularly
while parading in Paris on 14 July (Bastille Day). Because of the impressively
slow pace, which Legionnaires refer to as the "crawl", the Legion is always
the last unit marching in any parade. The Legion is normally accompanied
by its own band which traditionally plays the march of any one of the regiments
comprising the Legion, except that of the unit actually on parade. The
regimental song of each unit and "Le Boudin" (commonly called the blood
sausage or black pudding song) is sung by Legionnaires standing at attention.
Also, because the Legion must always stay together, it doesn't break formation
into two when approaching the presidential grandstand, as other French
military units do, in order to preserve the unity of the Legion.
Contrary to popular belief, the adoption of the Legion's slow marching
speed was not due to a need to preserve energy and fluids during long marches
under the hot Algerian sun. Its exact origins are somewhat unclear, but
the official explanation is that although the pace regulation does not
seem to have been instituted before 1945, it hails back to the slow, majestic
marching pace of the Ancien Régime, and its reintroduction was a
"return to traditional roots".
Calvin Coolidge's son
On 30 June 1924, Coolidge's two sons, John and Calvin Jr., set out to play
tennis on the White House tennis court. 16-year-old Calvin Jr., in a hurry
to get out on the court, donned tennis shoes but no socks. Young Calvin's
sockless exertions raised a blister on one of the toes on his right foot.
He didn't tell anyone, and it soon became infected. The next day, the 16-year-old
awoke with a stiff and painful leg. The doctor was called, and his examination
revealed that a septic infection had spread to Calvin's bloodstream and
throughout his body. In 1924, penicillin and other revolutionary infection-fighting
drugs were yet to be discovered, and Calvin's condition was critical. During
the next several days, seven doctors tried stomach washings, blood transfusions,
an operation, and other methods in desperate efforts to save the teenager.
But Calvin only grew weaker. By July 7, he was delirious. Finally, his
body began to relax. He said weakly, "I surrender," and lapsed into a coma.
Four hours later, at 10:30 p.m., he died. President Coolidge blamed himself
for his son's death, and many have claimed that it plunged him into a depression
from which he never recovered.
The strange death of such a prominent young man naturally attracted
the attention of the nation. Before long a rumor began circulating (particularly
among teenagers) that Calvin Jr.'s death was caused by the dye from his
black socks entering his bloodstream through a cut and poisoning him.
How this rumor began is something we can only guess at, and no obvious
explanations spring to mind. Obviously the public knew that whatever killed
Calvin had something to do with a wound on his foot and blood poisoning,
so perhaps the sock rumor arose because it seemed like a logical explanation
to those who were not privy to the details of his injury. Or perhaps, as
Morgan and Tucker suggest, it may simply have been "the result of youthful
anxiety about dress and appearance." Either way, the rumor may have seemed
plausible at the time because some of the coloring agents commonly used
by the clothing industry (such as zinc chloride, which was used to give
socks a pearl gray color, and aniline dye, which was used to make shoe
leather black) did indeed often cause serious inflammations when the unabsorbed
chemicals came into contact with a wearer's skin.
There appears to be a higher than average rate of divorce, alcoholism,
and premature death among the lives of children of U.S. Presidents.
Doug Wead (2002) All The Presidents' Children, Atria Books
John Tyler (President of USA, 1841·1845)
While a 30 year old Congressman in Washington, Tyler developed an
illness that remains difficult to diagnose. Based on Tyler's clear description
of the illness it would today be described as a symmetric, generalized,
subacute paralysis. His recovery was so slow and prolonged that he resigned
from Congress for two years.
Tyler described the illness to his doctor as follows:
I sustained a violent singular shock four days ago. I had gone to the house
on Thursday morning before experiencing a
disagreeable sensation in my head, which increased so much as to force
me to leave the hall. It then visited in succession hands,
feet, tongue, and lips, creating in each the effect that is produced by
what is commonly called a sleeping hand, which all of us are
subject to; but it was so severe as to render my limbs, tongue, and so
forth, almost useless to me. I was bled and took purgatives
which have rendered me convalescent. The doctor ascribed it to a diseased
stomach, and very probably correctly did so. I am
now walking about and I'm to all appearances well, but often experience
a glow in my face and over the whole system which is
often followed by debility with pain in my neck and arms.
Possible diagnoses include Guillain-Barre syndrome, myasthenia gravis,
tick paralysis, diphtheritic paralysis, and botulism
Bumgarner, John R. The Health of the Presidents: The 41 United States
Presidents Through 1993 from a Physician's Point of View. Jefferson, NC:
MacFarland & Company, 1994. ISBN 0-89950-956-8 [a] p. 64
[b] pp. 64-65 [c] p. 65
Dr. Samuel Mudd
and John Wilkes Booth's leg fracture
 After
he shot President Abraham Lincoln, John Wilkes Booth broke his left leg
in his leap to the stage at Ford's Theatre. Needing a doctor's assistance,
he and David Herold arrived at Dr. Mudd's (about 30 miles from Washington)
at approximately 4:00 A.M. on April 15, 1865. Dr. Mudd set, splinted, and
bandaged the broken leg (a fracture of the tibia & fibula 3 inches
above the ankle joint). The National Park Service photograph to the right
shows Booth's boot which Dr. Mudd removed when he treated the leg. Although
he had met Booth on at least three prior occasions, Dr. Mudd said he did
not recognize his patient. He said the two used the names "Tyson" and "Henston."
Booth and Herold stayed at the Mudd residence until the next afternoon
(roughly a 12 hour stay). Mudd asked his handyman, John Best, to make a
pair of rough crutches for Booth. Mudd was paid $25 for his services. Booth
and Herold left in the direction of Zekiah Swamp.
After
he shot President Abraham Lincoln, John Wilkes Booth broke his left leg
in his leap to the stage at Ford's Theatre. Needing a doctor's assistance,
he and David Herold arrived at Dr. Mudd's (about 30 miles from Washington)
at approximately 4:00 A.M. on April 15, 1865. Dr. Mudd set, splinted, and
bandaged the broken leg (a fracture of the tibia & fibula 3 inches
above the ankle joint). The National Park Service photograph to the right
shows Booth's boot which Dr. Mudd removed when he treated the leg. Although
he had met Booth on at least three prior occasions, Dr. Mudd said he did
not recognize his patient. He said the two used the names "Tyson" and "Henston."
Booth and Herold stayed at the Mudd residence until the next afternoon
(roughly a 12 hour stay). Mudd asked his handyman, John Best, to make a
pair of rough crutches for Booth. Mudd was paid $25 for his services. Booth
and Herold left in the direction of Zekiah Swamp.
Within days Dr. Mudd was under arrest by the United States Government.
He was charged with conspiracy and with harboring Booth and Herold during
their escape. He went on trial along with Lewis Powell (Paine), George
Atzerodt, Mary Surratt, David Herold, Ned Spangler, Samuel Arnold, and
Michael O'Laughlen. In court witnesses described Dr. Mudd as the most attentive
of the accused. He was dressed in a black suit with a clean white shirt.
Testimony against the doctor at the trial included his harsh treatment
of some of his slaves. He shot one male slave (who survived). New information
regarding Dr. Mudd surfaced in 1977. A previously unknown statement by
conspirator George Atzerodt indicated that John Wilkes Booth had sent liquor
and provisions to Dr. Mudd's home two weeks prior to the assassination.
Like the other defendants, Dr. Mudd was found guilty. His sentence: life
imprisonment. He missed the death penalty by one vote.
 Early in 1869
a courier from the United States Government knocked on the front door of
the Mudd farm. When Mrs. Mudd answered, the man handed her an envelope
and said, "From the President of the United States. Please sign this receipt
to certify that I have delivered it to you. If you have a reply, I shall
return it for you." Mrs. Mudd opened the envelope and found a letter written
on White House stationery. It read:
Early in 1869
a courier from the United States Government knocked on the front door of
the Mudd farm. When Mrs. Mudd answered, the man handed her an envelope
and said, "From the President of the United States. Please sign this receipt
to certify that I have delivered it to you. If you have a reply, I shall
return it for you." Mrs. Mudd opened the envelope and found a letter written
on White House stationery. It read:
Dear Mrs.
Mudd: As promised, I have drawn up a pardon for your husband, Dr. Samuel
A.
Mudd. Please
come to my office at your earliest convenience. I wish to sign it in your
presence
and give it to you personally.
Sincerely,
ANDREW JOHNSON
President
of the United States of America.
Mrs. Mudd went to the White House the next morning. There the President
signed and delivered to her the papers for
the release of her husband. The date of the pardon was February 8,
1869.
Dr. Mudd was released from Ft. Jefferson on March 8 and arrived home
on March 20. He had served somewhat less than
4 years in prison. He partially regained his medical practice and lived
a quiet life on the farm.
 Dr.
Mudd's father passed away in 1877. In January of 1878 Dr. Mudd's youngest
daughter and ninth child, Nettie, was
Dr.
Mudd's father passed away in 1877. In January of 1878 Dr. Mudd's youngest
daughter and ninth child, Nettie, was
born. In January of 1883 Dr. Mudd had a busy schedule with many sick
patients during a harsh winter. On New Year's
Day he put on his muffler and overshoes and called on patients. He
came down with a severe cold. He was running a
fever and had to remain in bed. As the days progressed, the fever rose.
On January 10th, 1883, Dr. Mudd died of
pneumonia or pleurisy at the age of 49. He was buried in St. Mary's
cemetery next to the Bryantown church where he
first met Booth in 1864. Sarah Frances, who was buried next to him,
lived until November 29, 1911. Dr. Mudd's
descendants, most notably Dr. Richard Mudd (1901-2002) of Saginaw,
Michigan, worked indefatigably to clear his name
of any complicity with John Wilkes Booth. Recently a petition (petitioner
Richard D. Mudd, M.D.) was filed in the United
States District Court for the District of Columbia (case No. 1:97CVO2946)
bringing suit against the Secretary of the Army,
Togo West et.al., ordering the Archivist of the United States to "...correct
the records in his possession by showing that
Dr. (Samuel A.) Mudd's conviction was set aside pursuant to action
taken under 10 U.S.C. sec. 1552.", and that the court
"...order the payment of Petitioner's costs in bringing this action;..."
On July 22, 1998, U.S. District Judge Paul Friedman
said he would rule soon, and on Thursday, October 29, 1998, he ordered
the Army to reconsider the conviction of Dr.
Mudd. Friedman said the Army's recent rulings (see below) against the
request were arbitrary. The following decision
was announced on March 9, 2000: SAGINAW, Mich. (AP) - The U.S. Army
has rejected an appeal to overturn the 1865
conviction of Dr. Samuel Mudd as an accomplice in the escape of John
Wilkes Booth after the Lincoln assassination.
Mudd's 99-year-old grandson, Dr. Richard Mudd of Saginaw, has waged
a long campaign to clear his grandfather's
name. But this week, Army Assistant Secretary Patrick T. Henry rejected
the latest request to throw out Samuel Mudd's
conviction by a military court. Henry said his decision was based on
a narrow question - whether a military court had
jurisdiction to try Samuel Mudd, who was a civilian. "I find that the
charges against Dr. Mudd (i.e., that he aided and
abetted President Lincoln's assassins) constituted a military offense,
rendering Dr. Mudd accountable for his conduct to
military authorities," he wrote in Monday's decision.
On March 14, 2001, Judge Friedman rejected Richard Mudd's contention
that his grandfather should not have been tried
by a military court because he was a citizen of Maryland, a state that
did not secede from the Union, and thus entitled to
a civil trial. John McHale, a Mudd family spokesman, said that an appeal
of Judge Friedman’s ruling would be filed. On
Friday, November 8, 2002, a federal
appeals court dismissed the case. Judge Harry Edwards wrote that the
law under
which the Mudd family was seeking to have Samuel Mudd's conspiracy
conviction expunged applied only to records
involving members of the military. Although Mudd was tried by a military
tribunal, he was not a member of the military.
Dr. Mudd, when under arrest for alleged complicity in Lincoln's murder,
had described Booth's
leg injury as "a straight fracture of the tibia about two inches above
the ankle. There was nothing resembling a compound fracture."(39)
In his letter to Secretary Stanton after the autopsy on Montauk, the Army
Surgeon General had stated that "the left leg and foot were encased
in an appliance of splints and bandages, upon the removal of which, a fracture
of the fibula (small bone of the leg) 3 inches above the ankle joint, accompanied
by considerable ecchymosis, was discovered."(40) In Montauk's pilothouse
that sultry April Thursday no questions had been asked about the leg. However,
shortly before his death in 1891 Dr. May composed a memoir in which
he attributed his identification of the body to "my mark. . .unmistakably
found by me upon it. Never in a human had a greater change taken
place. . .every vestige of resemblance to the living man had disappeared.
But the mark of the scalpel during life remained indelible in death"
settling once and for all "the identity of the man who had assassinated
the President." And the leg? "The right limb was greatly contused,
and perfectly black from a fracture of one of the long bones. . . ."
John Wilkes Booth's autopsy was performed aboard the Montauk by Surgeon
General Joseph K. Barnes and Dr. Joseph
Janvier Woodward. On April 27, 1865, Dr. Barnes wrote the following
account to Secretary of War Edwin Stanton:
Sir,
I have the honor to report that in compliance
with your orders, assisted by Dr. Woodward, USA, I made at 2 PM
this day, a postmortem examination of the
body of J. Wilkes Booth, lying on board the Monitor Montauk off
the Navy Yard.
The left leg and foot were encased in an
appliance of splints and bandages, upon the removal of which, a
fracture of the fibula (small bone of the
leg) 3 inches above the ankle joint, accompanied by considerable
ecchymosis, was discovered.
The cause of death was a gun shot wound
in the neck - the ball entering just behind the sterno-cleido muscle -
2 1/2 inches above the clavicle - passing
through the bony bridge of fourth and fifth cervical vertebrae -
severing the spinal chord (sic) and passing
out through the body of the sterno-cleido of right side, 3 inches
above the clavicle.
Paralysis of the entire body was immediate,
and all the horrors of consciousness of suffering and death must
have been present to the assassin during
the two hours he lingered.
Dr. Woodward wrote the following detailed account of his autopsy
on John Wilkes Booth:
Case JWB: Was killed April 26, 1865, by a conoidal
pistol ball, fired at the distance of a few yards, from a
cavalry revolver. The missile perforated the
base of the right lamina of the 4th lumbar vertebra, fracturing it
longitudinally and separating it by a fissure
from the spinous process, at the same time fracturing the 5th
vertebra through its pedicle, and involving
that transverse process. The projectile then transversed the spinal
canal almost horizontally but with a slight
inclination downward and backward, perforating the cord which
was found much torn and discolored with blood
(see Specimen 4087 Sect. I AMM). The ball then shattered the
bases of the left 4th and 5th laminae, driving
bony fragments among the muscles, and made its exit at the left
side of the neck, nearly opposite the point
of entrance. It avoided the 2nd and 3rd cervical nerves. These facts
were determined at autopsy which was made
on April 28. Immediately after the reception of the injury, there
was very general paralysis. The phrenic nerves
performed
their function, but the respiration was
diaphragmatic, of course, labored and slow.
Deglutition was impracticable, and one or two attempts at
articulation were unintelligible. Death, from
asphyxia, took place about two hours after the reception of the
injury.
Break a leg?
Although the Wilkes Booth story has been used to explain the Theater phrase
"Break a leg", the most plausible story behind holds that it originated
in twentieth-century Germany. Lexicographers believe the phrase comes from
the German Halsund Beinbruch (roughly, "break your neck and leg"), a phrase
first heard during World War I. Halsund Beinbruch was used in the Luftwaffe
as a way of saying happy landings, and it's still used in the theater and
among skiers.
American
Civil War Prosthetics: The Gettysburg Limb

In 1866, North Carolina became the first state to start a program
to give artificial limbs to thousands of amputees after the war.
The program offered free rail passage and rooming in Raleigh
to veterans who came to the city to have limbs fitted. The state paid $75
to those who didn't want an artificial leg or wanted to buy a different
model, and $50 to those who didn't want an artificial arm. In all, 1,550
veterans wrote to the state about their wartime disabilities.
Hanna, the peg-leg whittler -- like his grandson 137 years later --
thought the store-bought leg was something special. It was, Wegner says,
"his Sunday-go-to-meeting leg." Hanna, a native of Anson County, was a
member of the 26th North Carolina Regiment, a regiment that lost more soldiers
than any other on either side in the Civil War.
At Gettysburg on July 1, 1863, he was shot above the left ankle and
in the head. Surgeons removed the grapeshot from his head and amputated
his leg just below the knee. With arm and leg wounds, "They didn't take
shot out back then. They just whacked it off," said Hanna's grandson, Duncan
Hanna.
There was broad public support for the artificial-limb program, said
Ansley Herring Wegner, a researcher at the N.C. Division of Archives and
History. The state spent $81,310.12 on the program between 1866 to 1870,
she said. In 1872, the combined state and local budgets for public schools
was $155,000, according to state records. She has written a book on the
leg program titled "Phantom Pain" that will be published this summer.
Hanna agreed to lend his grandfather's leg to the state. After candy
wrappers, a dime and even a baby tooth were removed from inside, the leg
underwent some restoration work. It is now on display in a case at the
Bentonville Battlefield - next to the blades in a Civil War surgeon's amputation
kit.
"He liked to be sharp. He wouldn't wear it in the rain, either - not
even with a boot on it," he said. Robert Hanna struggled at times, especially
in the fall, when the corn stalks on his farm were dry. "You could hear
him screaming, and they'd say, 'Leave him alone,' " his grandson said.
"The wind would blow and the corn stalks would rub together and it would
sound like men marching. He'd have flashbacks." "He had one that had a
bull's hoof on it (for the foot)," his grandson said. Robert Hanna continued
using the state-issued leg sparingly until he died in 1918, still a proud
Confederate veteran.
"He was buried with no leg. He was buried in a gray uniform -
a gray suit they made for him. He wouldn't wear a blue suit," his grandson
said.
 Although
fortunate to be unconscious during surgery, soldiers who underwent the
knife often received a nasty visitor a few days later-infection. Any open
wound almost always became infected. The unwashed hands of the surgeon,
the non-sterile surgical instruments used on a succession of men, and the
dirty sponges used on an entire ward of wounded soldiers all introduced
infectious bacteria into wounds. These infections often resulted in gangrene
and death.
Although
fortunate to be unconscious during surgery, soldiers who underwent the
knife often received a nasty visitor a few days later-infection. Any open
wound almost always became infected. The unwashed hands of the surgeon,
the non-sterile surgical instruments used on a succession of men, and the
dirty sponges used on an entire ward of wounded soldiers all introduced
infectious bacteria into wounds. These infections often resulted in gangrene
and death.
Case of Private Julius Fabry
Private Julius Fabry, K Company,
4th U.S. Artillery, age 38, was shot in the left knee at the battle of
Deep Bottom, Virginia, on Aug.16, 1864. His leg was amputated just above
the knee on the following day. The thigh bone became infected and Fabry's
pain was treated with morphine for the next 6 years. Pus drained regularly
from the infected bone. In 1870, the infected bone was remove at the hip
joint. In 1878, Fabry reported no trouble with the stump, but he was unwilling
to use an artificial limb. Fabry died in 1894.
Amputation
 Surgeons
frequently treated arm and leg wounds by amputating. The grisly wounds
caused by bullets and schrapnel were often contaminated by clothing and
other debris. Cleaning such a wound was time-consuming and often ineffective.
However, amputation made a complex wound simple. Surgical manuals taught
that an amputation should be performed within the first two days following
injury. The death rate from these so-called primary amputations was lower
than the rate for amputations performed after the wound became infected.
Union surgeons performed nearly 30,000 amputations.
Surgeons
frequently treated arm and leg wounds by amputating. The grisly wounds
caused by bullets and schrapnel were often contaminated by clothing and
other debris. Cleaning such a wound was time-consuming and often ineffective.
However, amputation made a complex wound simple. Surgical manuals taught
that an amputation should be performed within the first two days following
injury. The death rate from these so-called primary amputations was lower
than the rate for amputations performed after the wound became infected.
Union surgeons performed nearly 30,000 amputations.
 Patients
undergoing amputation were first anesthetized. A tourniquet was applied
above the site of the proposed amputation. The skin and muscle were then
cut with amputation knives several inches above the fracture site. The
muscles were pulled up to expose the bone. An amputation saw was used to
cut through the bone. Once the cut was completed, large arteries were pulled
out from the stump tissue with a tenaculum and tied off to prevent bleeding.
The skin muscle was then released and the tissue sutured. Two types of
amputation were commonly used. A circular amputation involved cutting straight
through the skin to the bone and resulted in a stump that was circular
in appearance. A flap amputation required the tissue to be cut leaving
two flaps of skin that were used to create a stump. Fingers and other small
bones were amputated using the smaller metacarpal saw.
Patients
undergoing amputation were first anesthetized. A tourniquet was applied
above the site of the proposed amputation. The skin and muscle were then
cut with amputation knives several inches above the fracture site. The
muscles were pulled up to expose the bone. An amputation saw was used to
cut through the bone. Once the cut was completed, large arteries were pulled
out from the stump tissue with a tenaculum and tied off to prevent bleeding.
The skin muscle was then released and the tissue sutured. Two types of
amputation were commonly used. A circular amputation involved cutting straight
through the skin to the bone and resulted in a stump that was circular
in appearance. A flap amputation required the tissue to be cut leaving
two flaps of skin that were used to create a stump. Fingers and other small
bones were amputated using the smaller metacarpal saw.
Prosthetic limbs were designed
and built to help amputees regain some of their former capabilities. Some
of these devices were custom-made while others were mass-produced.
The Case of Private Columbus
Rush
Private Columbus Rush, Company
C, 21st Georgia, age 22, was wounded during the assault on Fort Stedman,
Virginia, on March 25, 1865 by a shell fragment that fractured both the
right leg below the knee and the left kneecap. Both limbs were amputated
above the knees on the same day. He recovered quickly and was discharged
from Lincoln Hospital in Washington on Aug. 2, 1865. In 1866, while being
treated at St. Luke's Hospital in New York City, he was outfitted with
artificial limbs.
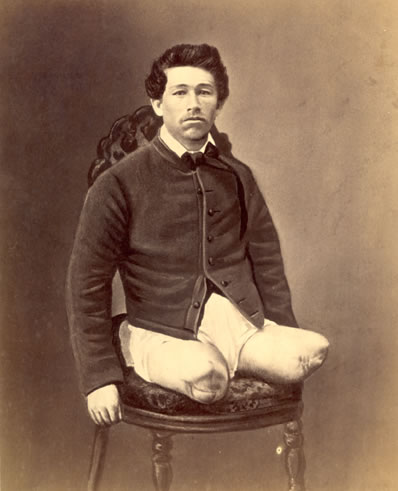 |
 |
| The results
of the double amputation. |
Using his
prosthetic legs, Rush could
walk with the aid of two canes. |
Excision
 Surgeons
treated some shoulder wounds with a technique known as excision, also termed
exsection or resection.
Surgeons
treated some shoulder wounds with a technique known as excision, also termed
exsection or resection. The fractured bone was removed, the tissues sutured, and the limb left
to heal. Excision gave the patient limited use of the arm and usually full
use of the hand. Prosthetic braces worn over the shoulder allowed nearly
normal function of the limb for some patients.
The fractured bone was removed, the tissues sutured, and the limb left
to heal. Excision gave the patient limited use of the arm and usually full
use of the hand. Prosthetic braces worn over the shoulder allowed nearly
normal function of the limb for some patients.
The Case of Private J.P. Kegerreis
Private J.P. Kegerreis, Company
B, 2nd Pennsylvania Heavy Artillery, was wounded at Petersburg, Va. on
June 17, 1864 by a minie ball. The ball entered his neck, punctured his
windpipe, and passed through his right shoulder joint and out his back.
Keggereis was tagged for amputation at the field hospital but tore off
the tag and crawled among the less seriously wounded. Three days later,
while at City Point Hospital, his wound was treated and found filled with
maggots. His neck wound healed in a month, but his shoulder wound was infected.
In the winter of 1865, the infected bone was removed by excision. The wound
healed slowly, and he was discharged in May of 1866. In December of 1867,
a surgeon removed a large piece of bone from the joint and the bones of
the arm later fused on a semi-flexed position. He was able to lift 135
pounds with his injured arm.
The Limping Lady of Baltimore
 Born
in 1906 in Baltimore, Maryland, Virginia Hall was a petite woman who loved
outdoor sports and thrived on skiing and hunting. Educated in economics
at Radcliff and then Barnard College in New York, she finished her studies
in Paris and Vienna. She was also fluent in French, German, and Italian.
In 1931, Virginia began what she thought would become a life-long career
in international relations. She took a clerk's position with the American
Embassy in Warsaw at a salary of $2,500 per year. Over the next few years
she would serve in Tallinn, Estonia; Vienna, Austria and Izmir, Turkey.
While hunting in Izmir her shotgun slipped from her grasp. When she grabbed
for it, the gun discharged and pellets struck her foot. By the time medical
help arrived, gangrene had already developed. The surgeon amputated her
leg to save her life. She was fitted with a B/K wooden prosthesis,
which she named "Cuthbert". The accident ended Virginia's plans for a long
career with the State Department. Not only did the State Department personnel
chiefs have a closed mind about women in the career service but there
also existed a regulation that disallowed employment of anyone with
"any amputation of a portion of a limb."
Born
in 1906 in Baltimore, Maryland, Virginia Hall was a petite woman who loved
outdoor sports and thrived on skiing and hunting. Educated in economics
at Radcliff and then Barnard College in New York, she finished her studies
in Paris and Vienna. She was also fluent in French, German, and Italian.
In 1931, Virginia began what she thought would become a life-long career
in international relations. She took a clerk's position with the American
Embassy in Warsaw at a salary of $2,500 per year. Over the next few years
she would serve in Tallinn, Estonia; Vienna, Austria and Izmir, Turkey.
While hunting in Izmir her shotgun slipped from her grasp. When she grabbed
for it, the gun discharged and pellets struck her foot. By the time medical
help arrived, gangrene had already developed. The surgeon amputated her
leg to save her life. She was fitted with a B/K wooden prosthesis,
which she named "Cuthbert". The accident ended Virginia's plans for a long
career with the State Department. Not only did the State Department personnel
chiefs have a closed mind about women in the career service but there
also existed a regulation that disallowed employment of anyone with
"any amputation of a portion of a limb."
She went to work istead for the British Special Operations Executive
in France in 1941-1942, operating with the "Maquis", the French Underground.
In 1941, as the Nazis were closing in on her, she escaped on foot over
the Pyrenees into Spain. Having become fluent in German and French as well
as Morse code during her tenure with the SOE, she joined the Office of
Strategic Services, or OSS, the World War II-era forerunner to the CIA,
in 1942, spying on the Germans using a milkmaid cover. The French Resistance
called her "la dame que boite," or the "Limping Lady." The Germans called
her "Artemis" and put her on the Gestapo's most-wanted list of Allied spies.
She had many Allied code names: "Bousey," "Marie Monin," "Germaine," "Diane,"
and "Camille."
The invasion of North Africa in November 1942 brought a torrent of German
troops into Vichy. Their sudden presence forced Hall to leave the country.
She crossed the Pyrenees mountains in the dead of winter. Before setting
out on the journey Virginia radioed SOE in London that she hoped 'Cuthbert'
would not be troublesome. London replied, "If Cuthbert troublesome eliminate
him." London had forgotten that 'Cuthbert' was the codename for her prosthesis!
The Gestapo attempted to capture the "woman with the limp" but were
unable to do so because of her exquisite disguise and the fact that she
had taught herself to walk with a "swinging" gait. She was instrumental
in collecting intelligence data, training Maquis in guerilla warfare and
sabotage, and actively participating in sabotaging German communications
during the D-Day Invasion. On a dark night in March 1944, Virginia Hall
strapped her wooden leg on her side and parachuted back into occupied France.
She set up voice and Morse code communications with the Allies and later
began to organize Free French Resistance operations and coordinated the
rescue and evacuation of downed Allied pilots. The Gestapo never caught
her.
Hall is the only civilian woman during World War II who received the
Distinguished Service Cross, the nation's second-highest military valor
award. She was honored with the MBE for her service after the Allied D-Day
invasion of Normandy on June 6, 1944. After the war, she became one of
the CIA's first female operations officers, breaking two glass ceilings:
the business of being female and the disability issue.
By Dr. Abraham Lieberman
Parkinson's disease may have been a key factor in Adolf Hitler's downfall.
The dictator suffered the disease, and the mental
inflexibility associated with it could have been what led
to his slow response to the D-Day landings in Normandy
in 1944, researchers said at the International Congress
on Parkinson's Disease in Vancouver.
Dr Tom Hutton, a neurologist who co-authored the study,
said Hitler was suffering physical and mental symptoms
of the disease, but his aides kept it secret.
He said that by the time of the Normandy landings, Hitler
had suffered the disease for 10 years and would have
had problems processing conflicting information - hence
his initial refusal to allow Panzer divisions to move to the
site of the invasion.
Hitler is said to have been convinced that the Allies
would launch their attack at Calais.
Debilitating disease
Parkinson's disease is a degenerative disease of the
nervous system that generally affects both men and
women who are more than 40 years old. However, 10%
of sufferers are believed to be under 40.
The disease develops slowly
and is associated with
trembling of the arms and
legs, stiffness and rigidity of
the muscles and slowness of
movement.
A third of Parkinson's suffers
also develop senile dementia.
In many cases, sufferers
eventually die from
secondary complications
such as pneumonia, urinary
tract infection, pressure sores, septicaemia and stroke.
It is thought to be caused by the death of nerve cells that
would normally produce a chemical - dopamine - that
carries messages around the nervous system.
"Hitler's slowness to counterattack at Normandy may
have been secondary to mental inflexibility and difficulty
in shifting concepts due to Parkinsonism," Dr Hutton's
discussion paper said.
Dr Hutton, of the Neurology Research and Education
Centre in Texas used records from officials who treated
Hitler in 1944 and 1945 that described him as having lost
"his mental flexibility".
Professor Max de Crinis established his diagnosis of Parkinson's disease
in
Hitler early in 1945 and informed the SS leadership, who decided to initiate
treatment with a specially prepared 'antiparkinsonian
mixture' to be administered by a physician. However, Hitler never received
the mixture, this implies that the SS intended to remove
the severely diseased 'Leader'. Two different character traits can be analysed
in Hitler's personality: on the one hand the typical
premorbid personality of parkinsonian patients with uncorrectable mental
rigidity, extreme inflexibility and insupportable pedantry. On
the other an antisocial personality disorder with lack of ethical and social
values, a deeply rooted tendency to betray others and to
deceive himself and uncontrollable emotional reactions. This special combination
in Hitler's personality resulted in the uncritical
conviction of his mission and an enormous driving for recognition. The
neuropsychiatric analysis of Hitler's personality could lead to a
better explanation of the pathological traits of one of the most conspicuous
historical personalities.
 Adolf Hitler had Parkinson disease! This surprises people. The reason
Adolf Hitler had Parkinson disease! This surprises people. The reason
they're surprised is that Hitler, the evilest-man of the 20th Century,
was
the most photographed man of the 20th Century. And, Parkinson, when it
appears, is easily recognized--and can be diagnosed on camera. So how
could the German public not know Hitler had PD? And how could the Allies:
England, Russia, and America, possessors of sophisticated secret-services
with thousand of cunning spies, not know Hitler had Parkinson disease?
Spies that penetrated each other's innermost circles, spies that knew
each other's innermost secrets --should've known Hitler had Parkinson
disease. Especially as the knowledge (in retrospect) is obvious from
watching films of Hitler. If an American President had Parkinson wouldn't
we know it? If a candidate for President had Parkinson wouldn't we know
it?
A German neurologist, Professor Max De Crinis, an advisor to Heinrich
Himmler, Chief of the SS, told Himmler, after watching films of Hitler,
that Hitler had Parkinson
disease. De Crinis never personally examined or treated Hitler. However,
the knowledge De Crinis
imparted to Himmler, that Hitler suffered from an incurable (and in the
1940s an untreatable) brain
disease was a factor in Himmler's betraying Hitler.
By 1940, shortly after World War II started, Hitler, his close associates,
and his doctors knew
Hitler was ill. In 1940, they may not have realized his illness was PD.
In a book, "Hitler's Fatal
Sickness and Other Secrets of the Nazi Leaders", Professor John Lattimer,
who in 1945 interviewed
and examined most of Hitler's associates, concluded that Hitler, shortly
after he started World War
II, knew he was ill, knew his time was limited, and wanted to fulfill his
plans before he was
incapacitated. Professor Lattimer's a renowned urologist and forensic pathologist--the
doctor
asked to review President John F Kennedy's autopsy.
In 1940 Hitler developed a tremor of his left-hand. After this he limited
his public appearances and
was rarely seen. And, he let himself be filmed only from angles that didn't
show his tremor. Tremor,
in the public mind, is erroneously associated with senility. And, neither
Hitler nor his associates
wanted anyone, neither the German public nor the Allies, to know Hitler
had a tremor. And,
perhaps was senile.
Evidence For Hitler's Parkinson's disease
1. Newsreels
Hitler's Parkinson's is most striking revealed in a 1945 Swedish newsreel.
The newsreel has been
reproduced on videotape and analyzed in an article for "Movement Disorders",
the official journal of
the International Movement Disorder Society. The 1945 Swedish newsreel,
unlike contemporary
German newsreels, escaped the German censors. The videotape shows Hitler
walking slowly, and
not swinging his left arm. He has a masked, dulled, expressionless face.
He walks slowly and
deliberately, not swinging his left-arm. He's stooped and bent-forward,
and he has an obvious
resting tremor of his left arm.
To diagnose Parkinson disease, patients must have at least two of Parkinson's
4 main symptoms:
resting tremor, slowness of movement, stiffness, and trouble walking. In
the newsreel Hitler has
the two most crucial symptoms needed for diagnosis: resting tremor, and
slowness of movement.
2. Photographs
Sometime in 1940, Hitler at age 51 years, became aware of a tremor of his
left hand. The tremor
was a resting tremor, one which appeared when the muscles of his hand relaxed
as opposed to
when they were contracted. Initially, Hitler's tremor was intermittent
appearing when he was
excited. He could usually hide his tremor by keeping his left-hand in his
pocket (picture 1), by
holding an object, a scroll, in his left hand (picture 2), or by cupping
his left hand over his right
(picture 3). Then later he cupped his right hand over his left (picture
4). As the disease advanced
, and was kept hidden from the German public, Hitler, nonetheless, became
more disabled (picture
5).
3. Eyewitness Reports
General H. Guderian, Hitler's Chief of Staff, wrote, in Guderian: Panzer
General that in February
1943: "Hitler's left hand trembled, his back was bent, and his gaze was
fixed."
Albert Speer, Hitler's architect and armaments minister wrote in Inside
the Third Reich: "In 1944
Hitler was shriveling up like an old man. His limbs trembled, he walked
stooped with dragging
footsteps.....His uniform, which in the-past he had kept scrupulously neat
was stained by the food
he had eaten with a shaking hands."
General von Cholitz, the German Commanding General in Paris said, upon
meeting Hitler in 1944:
"Hitler had become an old man. His face was worn..... His shoulders sagged.
He cupped his left
hand in his right to hide the trembling of his left arm. But above all,
it was his voice that shocked
me. The hard raucous voice had faded to a weak whisper."
G. Boldt, an intelligence officer on Hitler's staff, wrote in Hitler: The
Last Ten Days, An Eyewitness
Account, that in February 1945: "Hitler's left arm hung limply by his side,
and his left hand
trembled perceptibly.....He was not the vigorous, energetic Hitler the
Germans knew, the Hitler
that Goebbels, Minister for Propaganda, still depicted."
S. Knappe, an SS officer wrote in Soldat: Reflections of a German Soldier
that on meeting Hitler in
April 1945: "I was shocked by his appearance. He was stooped, and his left
arm was bent, and
shaking.....Both of his hands shook.....He looked.....at least twenty years
older than his 56 years."
4. Hitler's Handwriting
Hitler had micrographia, a small, compressed and cramped handwriting characteristic
of Parkinson
disease (picture 6).
5. Reports by Doctors Who Studied Hitler
Among the earliest, and best reports of Hitler's Parkinson disease, is
that by P. Stolk, a Dutch
authority (Professor Stolk never examined Hitler): "Hitler developed a
tremor, which affected only
his left-side. It was first noticed in his left-arm (in the autumn of 1942)
and subsequently also in
his left-leg. It's possible that his tremor had developed much earlier
(in 1940). His left-arm was
kept hanging down trembling heavily, or was pressed against his body, and
he dragged his left-leg.
The upper part of his body tended to incline forward. And finally he was
unable to walk without
supporting himself. In fact it was for this purpose that he had benches
placed against the wall of
the great bunker which was his retreat. Standing-up Hitler was (often)
forced to grab-hold of his
partner in conversation for support. His speech was low pitched and hardly
intelligible. His facial
expression became rigid and mask-like and saliva occasionally escaped from
the corner of his
mouth. In his final years Adolf Hitler evidently was suffering from Parkinson
disease."
Hitler's Symptoms
1. Slowness or Lack of Movement (Bradykinesia)
Bradykinesia (slowness or lack of movement) in Hitler, manifested itself
as decreased (or absent)
movement of Hitler's left-arm. This is first apparent in Leni Reifenstahl's
1934 film, Triumph of the
Will made during the 2nd Annual Nazi Party Congress in Nurnberg. The decreased
(or absent)
movement of Hitler's left arm, in the Reifenstahl film, is apparent when
Hitler's walking, or-talking,
automatic activities that don't require conscious awareness. Such patients,
including Hitler, can
move the affected arm when asked to do so: they are not paralyzed.
2. Tremor
Tremor is variable--and it's not always present. Indeed, 30% of all Parkinson
patients don't have
tremor. In Parkinson disease tremor, when present, begins on one side (as
in Hitler) and later,
after several years, spreads to the other side. The tremor may involve
the chin, but rarely the
head. The tremor is present when the arm is relaxed, hence the name, resting-tremor.
A
resting-tremor appears when Hitler's seated and his hand's supported, or
when he's walking and his
hand's hanging-down. The tremor usually disappears, when the patient innervates
the muscles of
his hand by making a fist or clenching an object.
Duration of Hitler's Parkinson's Disease
Dr. Abraham Lieberman, after a study of 300 hours of videotapes of Hitler,
from 1919 - 1940,
reported that the first symptom of Hitler's Parkinson disease, decreased
movement of his left-arm,
was apparent in 1934, when Hitler was 45 years old.
There are few clues as to the cause of Hitler's Parkinsonism,
although some have suggested it was post-encephalitic, while amphetamine
abuse is another possibility.
Lieberman
A (1997) .Hitler's Parkinson's disease began in 1933. Mov Disord 12(2):239-40.
Gerstenbrand
F, Karamat E.(1999) Adolf Hitler's Parkinson's disease and an attempt to
analyse his personality structure.Eur J Neurol. 6(2):121-7.
The Lockstep

Let the avenue to this house be rendered difficult and gloomy by
mountains and morasses. Let the doors be of iron, and let the grating,
occasioned by opening and shutting them, be increased by an echo that shall
deeply pierce the soul.
Dr. Benjamin Rush, Quaker reformer, 1787
 During
the early years of the 19th century, the reform-minded Quakers tirelessly
lobbied the Pennsylvania legislature to build a prison based on the idea
of reform through solitude and reflection. The Quakers hopefully and naively
assumed that an inmate's conscience, given enough time alone, would make
him penitent (hence the new word, 'penitentiary'). They wanted a new prison
to prove their theory, and in 1822 the Pennsylvania legislature approved
the funding. Penitentiary means literally a place for penitents, dating
from 1790, "when the Quaker state of Pennsylvania built a special cell
block to separate more serious offenders from lesser ones…" "Pen" for short.
During
the early years of the 19th century, the reform-minded Quakers tirelessly
lobbied the Pennsylvania legislature to build a prison based on the idea
of reform through solitude and reflection. The Quakers hopefully and naively
assumed that an inmate's conscience, given enough time alone, would make
him penitent (hence the new word, 'penitentiary'). They wanted a new prison
to prove their theory, and in 1822 the Pennsylvania legislature approved
the funding. Penitentiary means literally a place for penitents, dating
from 1790, "when the Quaker state of Pennsylvania built a special cell
block to separate more serious offenders from lesser ones…" "Pen" for short.
 The
inmates were not allowed to communicate with each other or meet for any
purpose, not even for religious services. Ministers sermonized to the inmates
while walking through the prison, their voices echoing through the cellblocks.
The inmates weren't allowed to sing, whistle, have visitors, see a newspaper,
or hear from any source about the outside world. They were allowed in their
exercise yards, which were attached to their 8 by 12 foot cells, just one
hour per day. At Eastern State, you went into your cell and you stayed
there. You saw no one except a guard, and you spoke to no one.
The
inmates were not allowed to communicate with each other or meet for any
purpose, not even for religious services. Ministers sermonized to the inmates
while walking through the prison, their voices echoing through the cellblocks.
The inmates weren't allowed to sing, whistle, have visitors, see a newspaper,
or hear from any source about the outside world. They were allowed in their
exercise yards, which were attached to their 8 by 12 foot cells, just one
hour per day. At Eastern State, you went into your cell and you stayed
there. You saw no one except a guard, and you spoke to no one.
 Here's how
the Quakers explained this policy: "No prisoner is seen by another after
he enters the wall. When the years of confinement have passed, his old
associates in crime will be scattered over the earth, or in the grave and
the prisoner can go forth into a new and industrious life, where his previous
misdeeds are unknown."
Here's how
the Quakers explained this policy: "No prisoner is seen by another after
he enters the wall. When the years of confinement have passed, his old
associates in crime will be scattered over the earth, or in the grave and
the prisoner can go forth into a new and industrious life, where his previous
misdeeds are unknown."
Although the Quakers banned flogging at the prison, other types of corporal
punishment were used. If you were caught communicating with another inmate
by, say, tapping on a pipe, you might be denied a few meals or secluded
in a dark empty cell for a day or two. The "shower bath" was another punishment
used at the prison. An inmate was stripped to the waist, chained to an
outside wall in cold weather, and doused with cold water. If it was cold
enough outside, ice would form on the inmate's body. Even crueler was the
"iron gag." This was a five-inch piece of metal that fit over the inmate's
tongue. The inmate was also cuffed with his wrists behind him, and a chain
was connected from the gag to the cuffs. If the inmate fought the device
and pulled with his arms, the gag was forced deeper into his mouth. At
least one inmate died from the iron gag.
The lockstep was introduced at Sing Sing Penitentiary ("Big House"),
Westchester County, New York. As well as being humiliating, it was also
often painful because prisoners were usually issued with tshoes that were
too tight. Many committed suicide because of the pain.


Inmate stripes pre-1904: One stripe for first timers, 2 for second offenders
and 3 for even more frequent repeaters. Right -- Inmate solid grays begin
1904.
The lockstep was abolished on August 9, 1900, and the striped uniform
went the same way four years later. Inmates were gradually permitted "freedom
of the yard" and baseball was introduced on the recreation field.
Charles Dickens visited the Eastern State Penitentiary in 1842 and later
wrote about it. "The System is rigid, strict and hopeless ... and I believe
it to be cruel and wrong.... I hold this slow and daily tampering with
the mysteries of the brain, to be immeasurably worse than any torture of
the body."
Images of America: Sing Sing Prison, Guy Cheli
Dr. Scholl


Foot
Doctor to the World, William H. Scholl.
Bob Marley's foot
In 1977, doctors diagnosed Marley with skin cancer. The singer had developed
melanoma in the big toe of his right foot, first noticed when a football
(soccer) injury refused to heal. Bob was playing football for hours a day.
Maybe we should ban soccer? For religious reasons Bob refused to have his
toe amputated and the cancer metastasised to his brain. He survived more
than two years with his cancer, not helped by the unorthodox medical treatment
of a Dr. Issel in Bavaria.
Bob Marley contemplating his own B/K amputation in an old aircraft
hangar that had been converted to an artificial limb factory (Heidelburg
1977).
You have to admit that it's kind of strange. They were playing football
and there was also this artificial limb factory in this big hall. Kate
Simon
One conspiracy theory maintains that the CIA killed Bob by putting a
copper wore in a boot which they sent to him and he tried on. When he put
his foot in the boot the wire stabbed into his toe injecting him with cancer.
Bob Marley,
The Photographs of Kate Simon (2003) Genesis Publications Ltd. UK
Nikita Khruschev
 The October 1960 shoe-banging
incident at the United Nations, which many Americans living during the
Cold War still remember. Khrushchev, though, had a good reason to be angry,
according to his grandson. Soviet Premier Nikita Sergeivich Khrushchev
pledged support for "wars of national liberation" in an address to the
United Nations in New York, At one point during the speech, Khrushchev
took off his shoe and banged it on the table. (One of his biographers speculated
that this was designed to improve his image at home.) Khrushchev came to
New York in the middle of the 1960 Presidential election campaign. His
U.N address awakened Western fears that he planned to aid Communist revolutionary
movements around the world. After his U.N. speech, Fidel Castro, leader
of the recent revolution in Cuba, visited Khrushchev in his hotel room.
The October 1960 shoe-banging
incident at the United Nations, which many Americans living during the
Cold War still remember. Khrushchev, though, had a good reason to be angry,
according to his grandson. Soviet Premier Nikita Sergeivich Khrushchev
pledged support for "wars of national liberation" in an address to the
United Nations in New York, At one point during the speech, Khrushchev
took off his shoe and banged it on the table. (One of his biographers speculated
that this was designed to improve his image at home.) Khrushchev came to
New York in the middle of the 1960 Presidential election campaign. His
U.N address awakened Western fears that he planned to aid Communist revolutionary
movements around the world. After his U.N. speech, Fidel Castro, leader
of the recent revolution in Cuba, visited Khrushchev in his hotel room.
 "The
main reason was that the representative of Indonesia told him that the
Soviet Union had slaves in Eastern Europe," Khrushchev said. "My grandfather
told him, `But you have slaves on some islands that are not belonging to
Indonesia.' They began to climb over the chairs.
"The
main reason was that the representative of Indonesia told him that the
Soviet Union had slaves in Eastern Europe," Khrushchev said. "My grandfather
told him, `But you have slaves on some islands that are not belonging to
Indonesia.' They began to climb over the chairs.
"Then my grandfather began to bang with his wrists and he lost his (watch)
on the floor. He began to look for it, then he found his shoe." As
a good performer, Khrushchev needed a strong, convincing exit, true to
the role he chose, and that is what happened: his shoes, made of durable
Soviet leather in a special shoe atelier for the Soviet nomenclature, were
too new and too tight, and he removed them. He bent down to pick up the
watch and saw his empty shoes. How lucky!
He sat up, and "one hand was with the shoe and one hand was without
the shoe. He was banging (the table) like a drum. Well, it turns out the
shoe may not have been banged, it may only have been brandished."
"It was merely for 15 seconds," Khrushchev concluded, claiming his grandfather
was defending his country's honor, not trying to threaten the Western world.

“It was not a big deal to the Soviets,” says his son Sergei Khrushchev,
“but when I moved here, people started to ask.” Khrushchev, was prompted
by one of those queries to rummage through his garage, where he found a
few boxes of his father’s old shoes. A few years ago Sergei Khrushchev
donated his papers to the John Hay Library at Brown University (where he
now works). When curator Mark Brown arrived to sort them, the two men came
across the shoes in the garage. “Would you like my father’s shoes?” Khrushchev
asked.
 “The
shoes in John Hay Library are not The Shoes,” he says. “I found an AP photograph
of my father wearing sandals at the United Nations.” What happened, he
thinks, is this: “My father came from Moscow in ordinary shoes, but when
he got to New York it was hot, so he switched to sandals. It was those
sandals that he wore to the United Nations that day.” The sandals—“My father
had very small feet: size seven or eight, like a boy”—were eventually thrown
out. And so the shoes in the archives are ones Nikita brought with him
to New York but didn’t wear. “Ordinary shoes,” says Sergei. “So it
is nothing special. Nothing at all.”
“The
shoes in John Hay Library are not The Shoes,” he says. “I found an AP photograph
of my father wearing sandals at the United Nations.” What happened, he
thinks, is this: “My father came from Moscow in ordinary shoes, but when
he got to New York it was hot, so he switched to sandals. It was those
sandals that he wore to the United Nations that day.” The sandals—“My father
had very small feet: size seven or eight, like a boy”—were eventually thrown
out. And so the shoes in the archives are ones Nikita brought with him
to New York but didn’t wear. “Ordinary shoes,” says Sergei. “So it
is nothing special. Nothing at all.”
Yet it's possible, as Taubman suggests, to trace the Cuban crisis to
Khrushchev's sense of betrayal two years earlier, when President Eisenhower
recklessly allowed a U-2 espionage flight over the Russian-Pakistan border.
After all, Eisenhower himself once claimed that nothing would make him
"request authority to declare war more quickly than violation of our air
space by Soviet aircraft."
When Kennedy succeeded Ike, Khrushchev couldn't resist testing the younger
president while avenging himself on Eisenhower, by shipping nuclear missiles
to Cuba. "What if we throw a hedgehog down Uncle Sam's pants?" he suggested
to a colleague. This debacle led directly to the end of Khrushchev's political
career in 1964, after which he became a "non-person," essentially ostracized
by all but his immediate family.
After he was dismissed as premier in 1964, Khrushchev's name was not
officially mentioned for 20 years. As far as the authorities were concerned,
the incident had
never happened, and neither had Khrushchev.
The shoe itself wasn't mentioned in the US media until Wednesday 12
October 1960. The head of the Philippine delegation, Senator Lorenzo Sumulong,
expressed his surprise at the Soviet Union's concerns over western imperialism,
while it, in turn, swallowed the whole of eastern Europe. Khrushchev's
rage was beyond anything he had ever shown before. He called the poor Filipino
"a jerk, a stooge and a lackey of imperialism", then he put his shoe on
the desk and banged it.
Nina
Khrushcheva The case of Khrushchev's shoe.(Nikita Krushchev shoe banging
incident at United Nations) New Statesman Oct 2, 2000
The rules about which side of the road people drive on are clear, but there
are also less clear "rules" that govern how
pedestrians behave in relation to each other. These pedestrian rules
are not usually enforced by law (the recent proposal to
legislate a "fast lane" for walkers on Oxford Street in London notwithstanding)
but form a sort of "accepted practice" that is
followed most of the time, but not all of the time, and which many
people are not consciously aware of -- until they travel to a
country with a different standard practice and end up bumping into
people.
Keep right: Keeping right is the normal practice in the USA and Canada.
(Although there might be some regional variations:
one reader says that people in Idaho keep to the left.). People even
keep right when skating on Ottawa's 8-kilometer-long skating rink on the
Rideau Canal in the winter. France also keeps to the right. Pedestrians
in Taiwan keep right and to reinforce the rule, some crosswalks in Taipei
had arrows directing people to keep right when crossing roads. As the habit
has become more ingrained, these arrows have been gradually removed.
No preference: The United Kingdom seems not to have a preference as
to which side of the path to use when walking.
This puts the British at a disadvantage when they go to places where
there is a standard practice, because "they are unaware that there is a
convention and so do not instinctively follow it, so getting in the way
of roughly half of the people coming the other way and muttering about
how crowded it is."
This doesn't mean that the British bump into each other. They don't
use single-file traffic like other nationalities, but still manage
to negotiate their way effectively -- presumably using some form of
body language or other cues to maneuver. Foreigners in the
UK who are not tuned in to the signals try to play follow-the-leader
and end up bumping into people when the leader's route
turns out to be unpredictable. Conversely, British tourists in foreign
lands who don't realize that they are supposed to fall in line,
cut through traffic at odd places and get run down.
Keep left: People in Japan keep left when walking. If someone is coming
at you and you step to your right, they step to their left, and you stay
on a collision course. Mexicans fight the flow by trying to keep left in
Texas when everyone else keeps right. In Hong Kong there is a slight tendency
to walk on the left.
Spiral stairs
Although Australians normally keep left, the spiral stairs in the Ballieu
Library at the University of Melbourne have a sign saying "keep right."
This is apparently for safety reasons. The steps curve to the right, or
clockwise, as you climb them, and they are very narrow on the inside of
the curve. Narrow stairs are easier to climb than to descend, because people
usually put only the forefoot on a stair and don't use their heels. Therefore,
it is easier and safer to climb on the inside of the curve, and descend
on the outside where the stairs are wider, meaning that one should keep
to the right.
This discussion brought up the question, why do the stairs curve in
the direction that they do? Traditionally, they curve right or
clockwise as you climb them, because it was easiest for a knight with
a sword to defend a tower if they curved in that direction.
Spend a few minutes chasing freshmen up and down the Ballieu Library
staircase while waving your right arm about, and you
should soon be convinced that it is easier and more effective to brandish
a sword if your sword arm is towards the outside of
the curve. (Use of real swords is not recommended if you want to retain
your book-borrowing privileges.) So the owner of a
spiral stair will prefer to defend while facing counter-clockwise,
and to have unwanted guests approach in a clockwise
direction. We assume that most often, the unwanted guests will be trying
to climb rather than descend. All of this assumes a
right-handed swordsman, of course, and a staircase which is wrapped
around a central support of some kind. A staircase
which follows the inside wall of a structure and has open space in
the center would operate in reverse, as would a staircase
which is meant to be defended from below instead of from above. There
is at least one Scottish castle built by a family with a strong tendency
towards left-handedness, which has staircases curving the other way around.
Escalators and moving walkways
On escalators and moving walkways in places like airports and subways (metros)
in Europe and North America, people
usually keep to the right and allow others to overtake on the left:
"walk left, stand right." Nicholas Hodder confirms that
despite the fact that Londoners walk every which way on the surface,
they observe the "stand on the right" rule on escalators in
the Underground. He also mentions that while there are "signs asking
passengers to stand on the right on escalators, there are
also signs asking passengers to keep to the left when walking around
connecting tunnels in some of the busier stations... It's all a
bit of a mess really."
In Japan, people didn't walk on escalators or travelators at all until
recently, but impatient Tokyoites recently started the habit overtaking
on the right, while the less impatient stood on the left. At about the
same time, the City of Osaka started putting up signs saying 'stand on
the right, walk on the left', on the grounds that this is how it's done
abroad. So now there are two distinctly different habits set up within
the same country."
In Australia, the convention on escalators is stand left, walk right.
Until a few years ago, underground stations in Melbourne had signs saying
this. For some reason they took the signs away, but everyone still follows
the convention.
Revolving doors
Another interesting choice that pedestrians must make is which way to go
through a revolving door. In North America and
continental Europe, people keep to the right when they pass through
revolving doors, and the door rotates counter-clockwise
as viewed from above. In Australia and New Zealand, the situation is
reversed and people keep to the left. Iin Atlanta (USA), there is a restaurant
(the Tavern at Phipps) which has a "large antique revolving door at one
of the entrances. A prominent sign on the door reminds people to enter
to the left, and explains that the door was originally installed in London
in 1908."